Book review: Vaxxers
A book authored by two lead scientists who developed the AstraZeneca vaccine
Intro
In January 2020 I was on a holiday in China with my boyfriend. When we had boarded the plane to Shanghai a week earlier Coronavirus was barely on our radar. Things changed very quickly. We planned to stay for 14 days but by the tenth day into our vacation all non-essential stores were shut, buying masks required hours of searching, and the Chinese government sent a text informing everyone in our area that a major highway 2 hours from our hotel would be closed “indefinitely”. We decided to leave on the evening of Tuesday 28 January, and booked flights for Wednesday morning, 3 days before our original departure.

You know shit has hit the fan when even Starbucks is closed.
If we had waited for our original departure flight, which left on Saturday, we would have been at the airport in Shanghai when the news broke that the Australian government would not let non-Australians flying from China back into the country. As a New Zealander, I would not be allowed back into the country where I had worked and lived for the past 12 months.
By the end of March, Sydney was in lockdown. And almost all news sources were warning that developing a vaccine would take many years. This seemed reasonable to me at the time; new vaccines usually took at least ten years to develop and roll out. The fastest vaccine ever developed was the mumps vaccine in the 1960s and that took 4 years. Little did I know that at that time Oxford University scientists had already analyzed the virus genome, modified it so it was suitable for a vaccine, and were now in the process of growing enough vaccine-ready material to be able to conduct a clinical trial. The development of the first batch of the AstraZeneca vaccine was nearly complete.
Summary of the book
Vaxxers is a book that chronicles the effort to develop the AstraZeneca vaccine. But unlike most such books, which are written by a journalist based on interviews, Vaxxers was written by two scientists who lead the effort to create the vaccine, Sarah Gilbert and Catherine Green.
Their main motivation for writing the book was to make vaccine development seem less mysterious and humanize the scientists who developed the vaccine. Their hope was that this would allay fears about receiving a shot, so I was a bit concerned their PR-instincts would take over and the book would be rather bland. In some respects this was true, many sections of the book were targeted at people who were skeptical of vaccines in general. But they also went into great detail explaining what it was like to be in their shoes, racing to develop the vaccine. What were they actually doing day-to-day? How do you go from a sequence of Coronavirus genome on a computer to a working vaccine in a few months? What does it feel like to actually do that work when you know that every decision you make has enormous consequences for all of humanity but you are also in a race against the worst pandemic in living memory, so decisions have to be made quickly? I could feel that both Gilbert and Green were proud and excited to share with the reader exactly how they made the vaccine and what their day-to-day lives felt like during that time.
The vaccine technology
Before I read the book I thought that the AZ vaccine was made using old, traditional methods, in contrast to the mRNA vaccines which were a new, general purpose technology.
It turns out this was not true. The method used to create the AZ vaccine is made using a “platform technology” - you can create a vaccine for any virus using the same technology (whether or not it is effective is a different story). The basic idea is to get the genome for COVID-19 virus, identify the part you want (the spike-protein part), do a few minor modifications (on a computer) and then send that data to a commercial lab. It only takes around two weeks (!!) for them to manufacture and send back a test tube with 100 billion real strands of DNA. You then combine that DNA with a non-replicating version of an chimpanzee Adenovirus and voila! You have the active ingredient in the vaccine. It then took another few months for the Oxford scientists to produce enough of it to conduct clinical trials.
Ebola
The Oxford scientists actually used this exact technology to create a vaccine for Ebola in 2014. Unfortunately, the vaccine never got to Phase III clinical trials. Ironically the concern was not that the vaccine would be unsafe, the concern was that in order to conduct a randomised controlled trial you need to give a placebo to half the participants, and by this time Ebola was so bad that it was argued (by the WHO I think?) it would be unethical to give people a placebo. The Oxford scientists were unimpressed with these arguments:
Anyone taking part in the trial would be closely monitored and, if infected, would receive care as early as possible, thus improving their chances further. And, the longer discussions about ethical trial design went on, the longer no one was receiving a vaccine that gave them any chance of protection at all.
Instead they used a “ring vaccination study” where the participants for the clinical trial are chosen in a different way and everyone in the clinical trial gets the vaccine, but some people in the trial get it later than others:
So instead, another type of trial design was eventually decided upon: a ring vaccination study with delayed vaccination in half of the rings. In order to use this type of trial design it is necessary to first identify someone who has been infected with Ebola. Then all of that person’s contacts are identified, and the contacts of their contacts, and the limits of the geographical area where they can be found are defined. That group of people forms a ‘ring’ around the initial case. Many rings are identified in this way, and each ring is randomly assigned to receive either immediate vaccination or delayed vaccination.
I don’t really see how this avoids the ethical concerns. Everybody who is not in the clinical trial is still given nothing and the more complicated trial design combined with the back and forth trying to nail down an acceptable trial design just delayed the vaccine even more.
Whilst all of the discussions about how to conduct the phase III trials had been going on, so had the Ebola crisis. It was frustrating to see the process slow down dramatically when a vaccine was so desperately needed…. by April 2015 when the ring vaccination study started – a full year after the outbreak became widespread – the case numbers were low and falling.
By the time they got approval for the trial Ebola cases were low and there was only enough Ebola going around to test one vaccine. A vaccine developed by a different group was chosen and the Adenovirus-based vaccine was never tested for efficacy.
The Oxford scientists thought this delay was unacceptable. WHO had a different take.
Why did it take so long to test for efficacy? It was four months from the outcome of the phase II trials until the start of the phase III study. I made this point at a conference where I had been invited to speak about our vaccine trial, and received a rather angry response from a WHO representative who insisted that everything had been done as fast as possible. But the fault does not lie with individuals not doing their job properly in the thick of things. The problem was a lack of preparation. The fact was that the delays meant not only that it took longer to contain the deadly Ebola virus, but also that only one vaccine ended up being tested for efficacy – a vaccine that required very low temperature storage, making it difficult and expensive to use in hot countries.
The line “the fault does not lie with individuals but … lack of preparation” seems like a cop-out to me. I understand the impulse not to blame individuals and more preparation for Ebola-like events is justified. But the problem here was that WHO’s “ethical concerns’’ don’t really make sense. WHO’s behavior is better explained by thinking of them as a Vetocracy rather than an organization primarily concerned about ethics.
Developing a COVID vaccine
Anyway, the Oxford researchers had this vaccine technology but it had never been subjected to efficacy trials. Then the coronavirus came. Within 48 hours of the COVID-19 genome being released the Oxford group had figured out which part they needed, modified it slightly, and sent the sequence to a commercial company ThermoFisher, to be manufactured. Remarkably, it only takes around a fortnight for these companies to turn DNA sequences stored in a computer into a test tube with around 100 billion strands of real DNA. While waiting for the DNA to come back from ThermoFisher the Oxford scientists had made preparations for how they were going to manufacture the vaccine. The lab available to them had already been precommitted to other projects. Thankfully they decided to say (paraphrasing) “fuck it - we’ll figure out finances later”:
My other concern was financial. The CBF [the lab they worked in] is run like a small business within the university, and in order to operate it has to cover its costs of around £1.5 million a year by charging its clients – researchers like Sarah and Tess – who in turn have to apply for grants to fund their research. The projects that Sarah was asking me to delay or deprioritise were already agreed, and their funding was secure right through to manufacture. It would be a big risk to the CBF’s operation to drop those in favour of this new project, when it wasn’t at all clear where the money might come from to pay for any of it.
They tried two different methods to manufacture the vaccine in parallel. A rapid method which was less likely to work and a slower but more reliable method.
The rapid method was originally developed to help fight cancer. You get some mutated DNA from a tumor, create a vaccine, give it to a cancer patient and their immune system will learn to recognize the mutated DNA and attack it. A cancer patient’s own immune system could learn to attack the tumour. This immune response sometimes happens without pharmaceutical intervention so the mechanism could plausibly work, but you need a vaccine personalized for every cancer patient’s exact tumour mutation. The only way this would be economically viable is with very fast vaccine manufacture.
In both methods the basic process is the same. They inserted some of the adenovirus/COVID-19 DNA into human cells. Remarkably, these cells all originate from the kidney of a single fetus that was aborted in the Netherlands in the 1970s. These human cells have been sitting in labs replicating for the past 50 years.
These human cells start producing the virus that would become the main ingredient in the vaccines. It’s not exactly clear to me exactly why the virus can replicate in these cells but can not replicate when injected into my arm but I think it’s because they do a special procedure to get it inside the human cells.
They then carefully help these human cells replicate until they have enough of the virus. In the end they made 300mls of fluid with this virus. That cup of fluid was “destined to seed the manufacture of every dose of the Oxford vaccine ever produced.” (Imagine holding that in your hand knowing that if you break it your clumsiness could be measured in millions of lives.)
Sadly the rapid method did not work. Fortunately, the traditional one did. This was one example of a broader theme in the book where they tried many different things in parallel, fully expecting to have some “wasted” effort.
To move quickly, we would still perform all the same tests as usual, we just wouldn’t wait for the results before moving on to the next part of the process. If the starting material failed any of its tests, we would have to throw out anything we had made from it. But that risk – a risk of wasted time and effort and serious money, but not of quality – was one we were prepared to take.
The next few weeks were some of the most hectic and surreal of my life. I was running in parallel half a dozen stages of vaccine development that would usually happen over years and in sequence.
Because we had never used this method before, we also made preparations with lots of different conditions: different ratios of adenovirus DNA to spike protein DNA, different ratios of cells to DNA, and so on.
Thank God they appreciated early on just how important speed was.
Partnering with AstraZeneca
The Oxford group then had to partner with a company to scale up the manufacturing. Surprisingly, the scientist themselves did not have input into selecting the company.
But Andy’s email was the first time I heard mention that it would be AstraZeneca, and it was something of a surprise. I knew they were big in cancer medicines and they were obviously a name in the pharma world, but they did not have a particular reputation for vaccine manufacture. We felt a bit disconnected: as though decisions that would really affect our working lives (by this point all of us were working on this project all of the time and it had completely taken over every waking and sleeping hour) were being taken at the highest level of the university with no consultation with those of us who actually knew how to make this vaccine.
Working with a large multinational was the exact opposite of what they were used to: a close-knit group of scientists who all understood what everyone else was working on.
AstraZeneca is an enormous entity, with multiple teams across the UK and the US with quite specialised roles, whereas everyone at our end was involved in and knew about everything. Also, they had no experience of manufacturing viral vectors, so the technical aspects of producing viral vectors, and the quality tests needed for these kinds of products, were all new to them. It was frustrating to have to keep repeating ourselves to slightly different combinations of AstraZeneca people.
But the Oxford scientists did come to appreciate their corporate partners. Companies have certain strengths that tend to complement research scientists.
I remember being in a meeting very early on, probably in May, when someone at AstraZeneca confidently used the phrase ‘billions of doses’. That’s a real shock to the system when a really big day for you is manually putting 500 doses into vials. They were prepared to throw everything at it straightaway, rather than waiting for results from clinical trials before they fully invested.
Companies also just have way more money to spend. (Provided the benefit/cost ratio is high enough).
The vaccine was still in Italy, the trials were in the UK – and there were no commercial flights operating between the two. We were stuck. … It turns out chartering a private jet costs around £20,000, normally well beyond the budget of a small academic clinical trial. But by this time we had the might of a global pharma company behind us. All those meetings with our AstraZeneca colleagues were starting to come good: we got permission to proceed. The jet arrived in London the next day with no passengers, just a large box of dry ice and 500 precious vials for next-day distribution across the UK. The trial must go on.
Clinical trials and regulatory agencies
The clinical trials were similar to clinical trials in normal times. Except that the gaps between the stage I, II and III trials were much smaller and all the data was processed much faster. Recruiting volunteers was also much easier.
The recruitment of volunteers to clinical trials is often quite a challenge…. [But] Within hours of announcing that we were recruiting volunteers for trials, we had thousands of applications.
The scientists praise the MHRA (the UK health regulator) in the book. They said the MHRA was quite cooperative and was willing to weigh the harms of using a slightly different process than usual against the benefits of manufacturing a vaccine faster. For example, there were some issues with the dosing in the Phase I trials and the MHRA was reasonably flexible. I take what the authors say with a pinch of salt because the MHRA acts as a gatekeeper for all their work. So it is probably unwise for them to heavily criticize the MHRA and sour their relationship with the very same people who they need to cooperate with for the rest of their careers. On the other hand, anecdotes like this are good evidence the praise is genuine:
The biggest risk (albeit a very small one) was that the Covid-19 vaccine might get contaminated with a bit of the previously manufactured product. We had a very sensitive and specific test for this valuable product, so we knew we would be able to test our final vaccine to check if there had been any contamination. Proceeding without fumigation would save at least three weeks. We drew up a formal risk assessment and submitted it to the Medicines and Healthcare products Regulatory Agency (MHRA, the body responsible for approving every step of our vaccine development process and ultimately for deciding whether to allow it to be used), who agreed our approach. (This was the first of a very large number of communications we would have with the MHRA over the coming months. That relationship, and the MHRA’s proactive approach, is a critical part of this story.)
Compare this to the FDA (the US health regulator). The FDA has been criticized heavily throughout the pandemic for being too biased in favor of inaction and inflexibly following pre-pandemic processes. This anecdote was telling:
The FDA approach was more process-driven, whereas the MHRA’s approach was more interactive, and more focused on gathering the evidence needed to assess the risks and answer the scientific questions. By way of illustration, many years previously we had been asked to collaborate with a US group working on malaria vaccine development. We had already completed a phase I clinical trial on a vaccine. It had been well tolerated, but – as happens a lot in vaccine development – the immune response was not as high as we had hoped, and we were not planning to proceed any further with it. But we did still have some of the batch left and the US group wanted to do a trial using our vaccine in combination with another one to see if that might improve the immune response. The issue we came up against was that although we had completed a clinical trial successfully in the UK, the FDA required toxicology studies to have been completed in two different species whereas in the UK we only have to complete a toxicology study in one species. We had done that and proceeded to human trials, and shown no safety concerns. On a call with the FDA, we explained that we had safety data from mice, and also from humans, which are a species after all, so would that work for them? The answer was no. They needed toxicology studies from another animal species – a rat or a rabbit. The problem was that if we did a toxicology study in rats or rabbits, it would use up the limited amount of vaccine that was remaining, and we wouldn’t then be able to do the clinical trial.
…
We were, however, unable to come to an agreement so the clinical trial was never carried out.
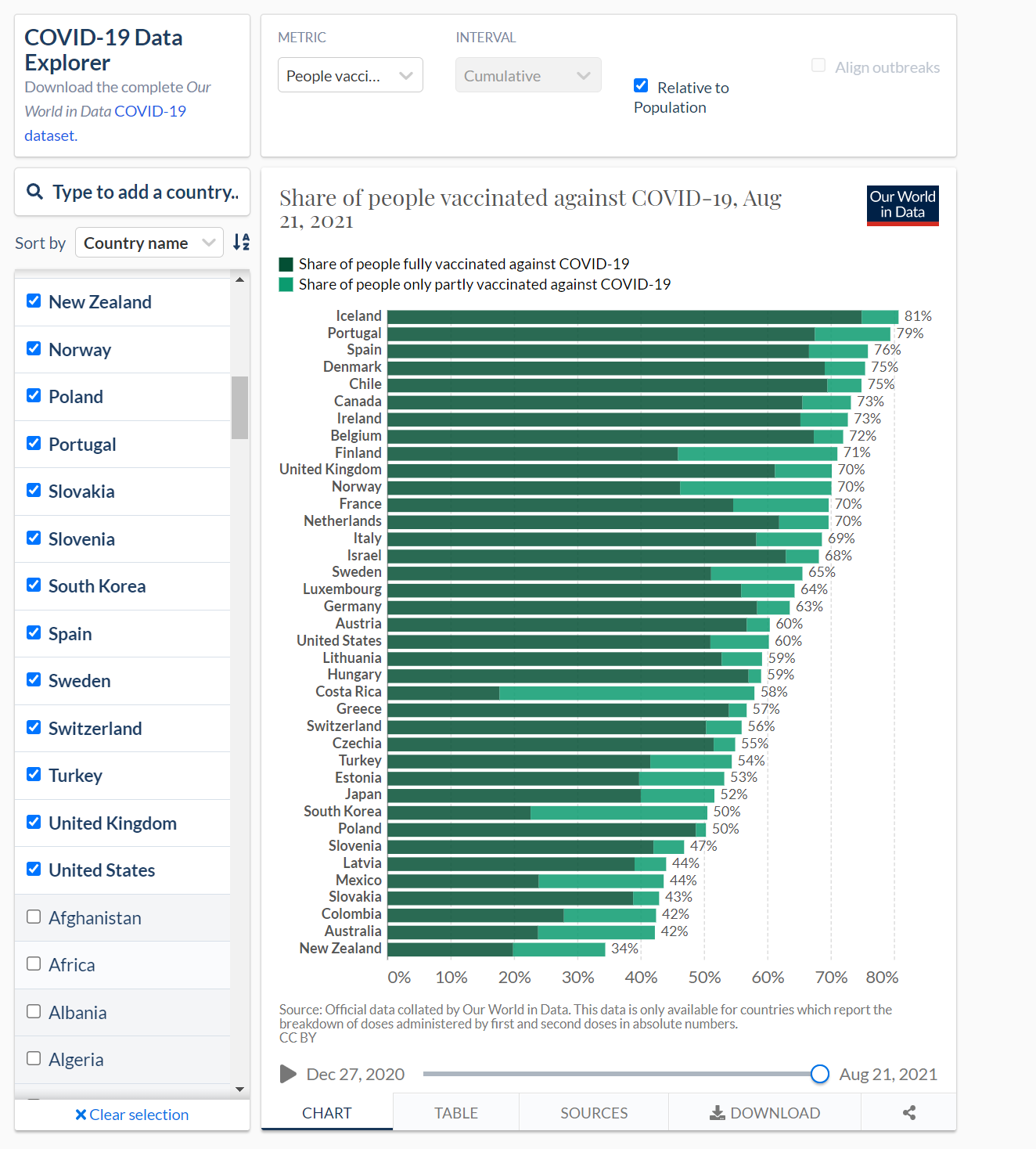
It was hard to read passages like the one above. The TGA (the Australian health regulator) has somehow been even slower than the FDA. As a result, I’m writing this during a lockdown in Australia where (as of Aug 21) our vaccination rate is lower than 36/38 OECD countries. These excerpts from an article by Steven Hamilton and Richard Holden give a summary for those of you who are unfamiliar with Australia:
{kind=link}
At the end of 2020, as vaccines were rolling out en masse in the Northern Hemisphere, the TGA [Therapeutic Goods Administration, AT] flatly refused to issue the emergency authorisations other regulators did. As a result, the TGA didn’t approve the Pfizer vaccine until January 25, more than six weeks after the US Food and Drug Administration (FDA), itself not exactly the poster child of expeditiousness.
Similarly, the TGA didn’t approve the AstraZeneca vaccine until February 16, almost seven weeks after the UK.
In case you’re wondering “what difference does six weeks make?“, think again. Were our rollout six weeks faster, the current Sydney outbreak would likely never have exploded, saving many lives and livelihoods. In the face of an exponentially spreading virus that has become twice as infectious, six weeks is an eternity. And, indeed, nothing has changed. The TGA approved the Moderna vaccine this week, eight months after the FDA.
It approved looser cold storage requirements for the Pfizer vaccine, which would allow the vaccine to be more widely distributed and reduce wastage, on April 8, six weeks after the FDA. And it approved the Pfizer vaccine for use by 12 to 15-year-olds on July 23, more than 10 weeks after the FDA.
Where’s the approval of the mix-and-match vaccine regimen, used to great effect in Canada, where AstraZeneca is combined with Pfizer to expand supply and increase efficacy? Where’s the guidance for those who’ve received two doses of AstraZeneca that they’ll be able to receive a Pfizer booster later?
But the slow, insular, and excessively cautious advice of our medical regulatory complex, which comprehensively failed to grasp the massive consequences of delay and inaction, must be right at the top of that list.
Conclusion
The book has great anecdotes from the scientists and delves into lots of other topics in detail:
- The media and political response to the vaccine, e.g. Macron said the vaccine “‘seems quasi-ineffective on people older than 65” based on a news article that claimed the vaccine was “only 8% effective” for old people. This was completely made up.
- The infamous dosing problem in the clinical trial.
- Security against anti-vax protestors.
- How much time scientists spend securing funding. Gilbert writes “Actually, raising funds had been my main activity for years”.
- Just how stressful this was for everyone involved.
Unfortunately there’s not that much discussion of the blood clot concerns because that was a relatively recent development. (Personally, I think those concerns are overblown and have been vaccinated with AZ myself.)
The take-home message of the book was that we need to be prepared to make vaccines for a pandemic (duh) and we need to be prepared to make them quickly. In particular, the authors suggest working on an annual flu vaccine development with the same emphasis on speed that we would expect in a pandemic. This can be used to validate that we have the capability to rapidly create a vaccine and scale up manufacturing before the next pandemic hits us.
For example, might it be cost-effective, given how much flu costs the economy, to work on flu vaccine development with as much urgency as we applied to the Covid vaccine? It would require more funding upfront, and the acceptance that not everything that was tried would work, but it might be the way to make some real progress rather than continuing to limp along as we have in the past, with small projects and no joined-up approach.
Most of the delay when creating the vaccine was logistical: securing funding, getting regulatory approval, conducting clinical trials and collaborating with multinational companies. An end-to-end test of rapid vaccine production, using the flu as a test case, is a great way to make sure every part of the pipeline can move quickly during a future pandemic. Besides, the normal flu is pretty deadly so we should arguably be putting a lot more money into fighting it anyway.